Health Economists often use the cost per quality-adjusted life year (QALY) metric to answer this question. QALYs are used to measure not only the additional years of life from a treatment, but also the quality of life. For instance, you may prefer to live 1 year in perfect health to two years in a coma. A QALY of 0.5 can indicate that the patient lived for 6 months in perfect health or for 1 year at a 50% health level.
Two popular methods to evaluate the value of a statistical life are stated preference and the value of a statistical life methods.
A first and direct approach is to ask respondents about their WTP for small health increases/QALYs using stated preference (SP) techniques such as discrete choice experiments or contingent valuation. The WTP estimates can subsequently be used to estimate the WTP for a gain in a full QALY. A second approach is to use the monetary value of preventing fatalities (the value of a statistical life), on which there is a substantial empirical literature, in order to implicitly derive the WTP-Q assuming a certain life expectancy (LE) and discount rate for the sample on which the value of life is derived.
Payers often used the cost per additional QALY to determine if a product is cost effective. Countries often only approve reimbursement for a therapy if the cost per QALY falls below a certain threshold. Ryen and Svensson (2014) write:
Threshold values often referred to in the literature and policy debates include the US value of US$50,000 to US$100,000 (approximately €37,500 to €75,000), which dates back to 1982 (Kaplan and Bush, 1982), and a UK threshold value around £20,000 to £30,000 (approximately €24,000 to €36,000) (NICE, 2004). In Sweden, relevant government authorities have suggested a threshold of 500,000 SEK (approximately €57,000) (Socialstyrelsen, 2007).1
The authors look at the literature on the value of a QALY and find significant variation across studies.
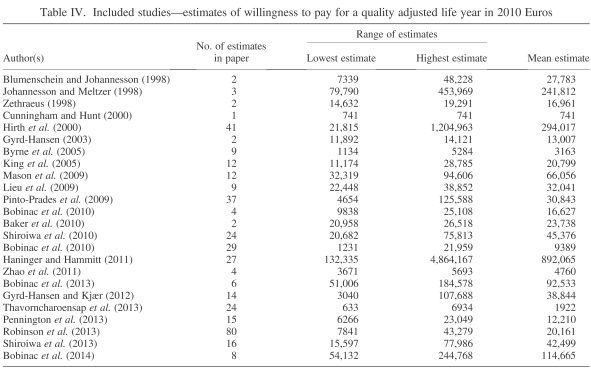
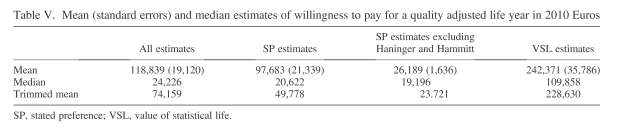
Overall, the average willingness to pay for a QUALY is 118,839 EUR 2010, which is equivalent to $179,000 USD in today’s dollars. The median WTP however, is only 24,226 EUR (or $36,000 in 2014 USD). Additionally, there is variation across method for valuing a life year. WTP measures using the stated preference measure are likely to be much smaller than those using the value of a statistical life (VSL) measure. Disregarding the 2.5% highest and lowest estimates, respectively, the resulting trimmed mean amounts to €74,159, or ($114,545 in 2014 USD)
Some additional conclusions from the authors:
We find that individuals have a higher WTP if the QALY is based on length of life improvements compared with QoL improvements. Further, the evidence indicates that there is a problem with scale bias, that is, WTP is not linearly proportional to the QALY change respondents are asked to value, which implies that WTP-Q is lower if respondents are asked to value higher changes in QALY.
Source:
- Ryen L. and Svensson M.(2014), THE WILLINGNESS TO PAY FOR A QUALITY ADJUSTED LIFE YEAR: A REVIEW OF THE EMPIRICAL LITERATURE, Health Econ., doi: 10.1002/hec.3085
3 Comments