In the United Kingdom, the National Institute for Health and Care Excellence (NICE) made an update to their health technology evaluations manual in January 2022. Of particular interest, section 6.2 of the manual states that the review committee “will consider the associated absolute and proportional QALY shortfall.” The committee defined QALY shortfall two ways:
- Absolute QALY shortfall. This quantity is defined as difference in the level of QALYs for individuals with the disease compared to individuals of the same age and sex distribution without the disease. In other words, if the number of QALYs for people with the disease was A and the number of QALYs to individuals with similar characteristics, but without the disease was B, then absoluate QALY shortfall is B-A.
- Proportional QALY shortfall. The proportional QALY shortfall is calculated by taking the absolute QALY shortfall and dividing this figure by the expected QALYs for individuals in the comparison group. From the example above, proportional QALY shortfall is calculated as (B-A)/B.
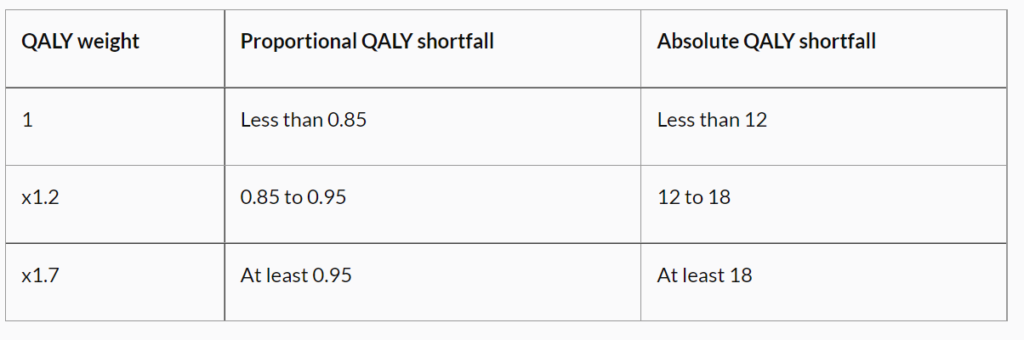
Once the proportional and absolute QALY shortfalls are calculated, NICE has proposed using specific QALY weightings as described in the table below. NICE intends to apply the severity multiplier only to therapeutic health technologies, but not diagnostic health technologies.
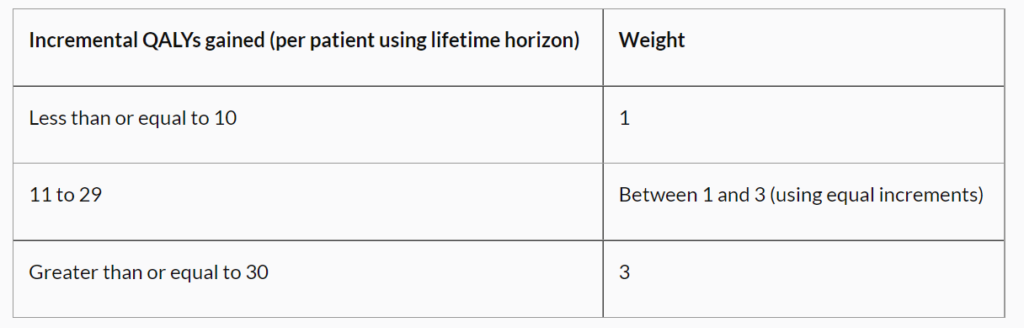
NICE also may consider increase in QALY weightings for highly specialized technologies (HST) with large incremental gains in QALY as measured over the lifetime time horizon of a new technology. The table below describes how these will be applied. While the application of these weightings is highly mechanical, identifying the shortfalls requires data analysis on the counterfactual of what the QALYs would be in the absence of disease
These two modifications aim to address two violations of constant QALY valuations as identified in
by Nielsen et al. 2021 among others: scope insensitivity and Severity independence.