The advent of treatment guidelines and pay-for-performance may be a good thing for the “average” patient. However, not all patients respond the same way to given treatments. Thus, just because a treatment benefits the average patient, does not mean that the treatment is beneficial for a given individual patient.
This phenomenon is known as treatment heterogeneity. Kravit, Duan and Braslow (2004) have a clear, concise, non-technical paper explaining this concept. The figure below describes how treatmetn heterogeneity affects outcomes. In Panel A, there is much more heterogeneity than Panel B. The probability a patient has a greater than 0 net treatment benefit is much higher in panel B than panel A. Panel C demonstrates that even in the presence of treatment heterogeneity, all else equal larger average treatment effects decrease the probability that individual patients will not benefit from the treatment. 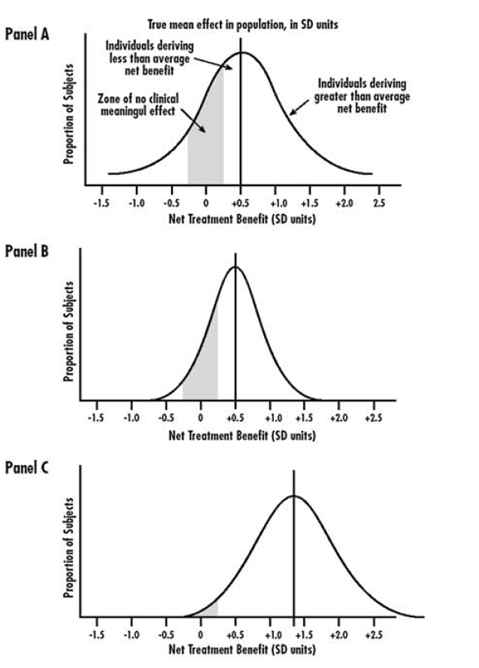 There are many sources of treatment heterogeneity. Some examples are below.
There are many sources of treatment heterogeneity. Some examples are below.
- Risk without Treatment (Baseline Risk). Coronary artery bypass surgery is lifesaving (reduces the risk of mortality) when performed on patients with blockage of the left main coronary artery (the major source of blood to the entire left side of the heart), but generally not when performed on patients with blockage of only one or two vessels
- Genetic Responsiveness. Among men with coronary atherosclerosis, carriers of two B1 alleles of the cholesteryl ester transfer protein benefit most from pravastatin. Further, 7 percent of Caucasians cannot metabolize codeine into morphine and so do not get any pain relief from codeine; breast cancer and lymphoma patients with one or more APO-E4 alleles are more likely to experience chemotherapy-related cognitive decline
- Responsiveness due to behavioral and environmental factors. For instance, patient adherence to prescribed treatment varies significantly.
- Vulnerability. Genetic and environmental variations in susceptibility to side effects can have a major impact on the net effect (benefit or harm) of treatment. A genetic marker predicting serious reactions to abacavir, a drug used to treat HIV infection. About 5 percent of patients treated with abacavir develop a serious, potentially life-threatening allergic reaction.
- Utilities. Patient preferences over outcomes differ. Some prostate cancer patients would be willing to give up only one year of life to avoid impotence and incontinence, but other patients would be willing to give up 10 years of life to avoid impotence and incontinence.
The authors conclude with the following words of advice for clinicians.
First, they should recognize that even compromised knowledge is better than complete ignorance. Thus, in the absence of information on HTE and ITEs, reliance on average effects as measured in good clinical studies is likely to produce better outcomes than is intuition or habit. Second, clinicians should seek evidence for or against the applicability of reported treatment effects to the patient at hand. How alike are the patient in the office and the average patient in the relevant clinical studies? Are there good reasons (empirical or pathophysiological) to believe that substantial HTE could exist? Third, physicians should try to assess their patients along the dimensions of susceptibility/prognosis, responsiveness, and vulnerability and to use their clinical judgment to integrate these concerns into a treatment recommendation.
Source:
- Richard Kravitz, Naihua Duan, and Joel Braslow. Evidence-Based Medicine, Heterogeneity of Treatment Effects, and the Trouble with Averages. Milbank Quarterly, Vol 82, No. 4, 2004 (pp. 661-687).