How does one select health state utilities used to populate a cost effectiveness model? This can be a challenge as outlined in Brazier et al. (2019):
Selecting evidence in an ad hoc manner results in unjustifiable conclusions and raises the possibility of cherry picking. For consistency within a model, utility data on all health states should be informed by evidence obtained from studies that used the same preference-based measure and preference weights, although this may not always be possible.
When multiple appropriate HSUs are available for a particular health state or when it is not possible to identify all HSUs from the same measure, it might be reasonable to synthesize (ie, combine) the data.
So what is a researcher to do? The 2019 ISPOR guidelines recommend the following:
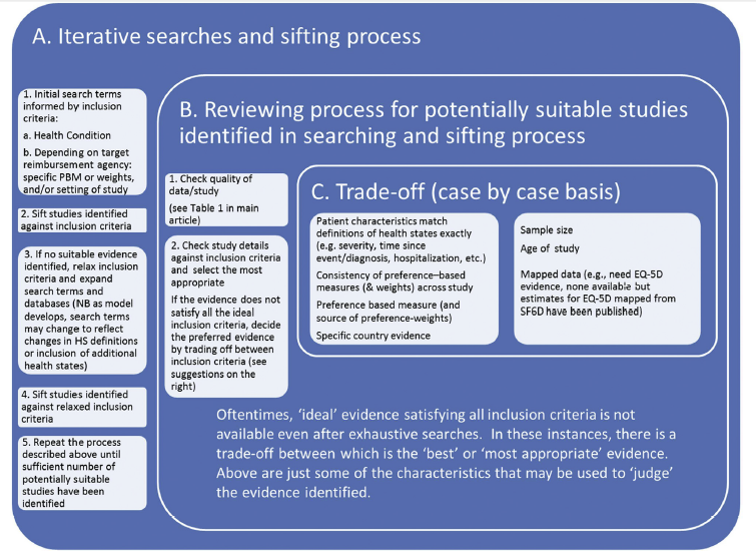
- Iterative searching. A single search is probably not enough because health state utilities come from trials, observational studies and previous economic analyses. Thus, an iterative approach is helpful. NICE outlines how to do this iterative approach. The figure below describes this process of iterative searching and sifting.
- Systematic searching. Ideally, the search for utilities would be systematic in nature. In many cases, however, a full SLR is not feasible within a studies resource constraints. Still, it is helpful to explicitly describe how the search was conducted to make sure the evidence identified was not done so opportunistically (i.e., cherry picking).
- Types of health state utilities. These can include health state utilities in the CEA model, treatment impact on utilties (from both an efficacy and safety [i.e., adverse event]) perspective, caregiver health state utilities, comorbidities, and moderator variables (i.e., method of administration or treatment setting).
- Databases to search. These may include MEDLINE and more specialized databases such as the TUFTS Database, ScHARRHUD, and HERC Mapping Database.
- Evidence synthesis. Typically a single study is used for a health state utility parameter based on study quality and appropriateness, but formal evidence synthesis techniques can be used, typically if there are 4 or more studies available. However, heterogeneity in study approach often makes formal evidence synthesis challenging. If there are a sufficient number of studies, meta-regression may be used to help control for heterogeneity in study populations.
- Evaluating study quality. Sample size, response rate, and rate of missing data/loss to follow-up will all affect the quality of the findings. Additionally, the study should be for a similar patient population describing a similar health state within that disease. The metric should be valid and sensitive to changes in health state.
- Reporting for reviews of health state utilities. The guildelines recommend using the Minimum Reporting Standards of Systematic Review of Utilities for Cost-Effectiveness (SpRUCE), which include documenting the search strategies used, the review process (who choose which studies to use, were there multiple reviewers, and how were disagreements handled), data extraction process and rationale for including the final utility values.
- Modelling utilities. A key modelling issue is whether there is an acute event where patients experience disutilities from their baseline health state over a fixed time duration or whether an event represents a transition to a new state with a corresponding new baseline utility level.
- Sensitivity analyses. Regardless of the evidence found, it is important to check how sensitive a CEA model is to health state utility values.
Source:
- Brazier J, Ara R, Azzabi I, Busschbach J, Chevrou-Séverac H, Crawford B, Cruz L, Karnon J, Lloyd A, Paisley S, Pickard AS. Identification, review, and use of health state utilities in cost-effectiveness models: an ISPOR good practices for outcomes research task force report. Value in Health. 2019 Mar 1;22(3):267-75.
1 Comment